Abstract
Background
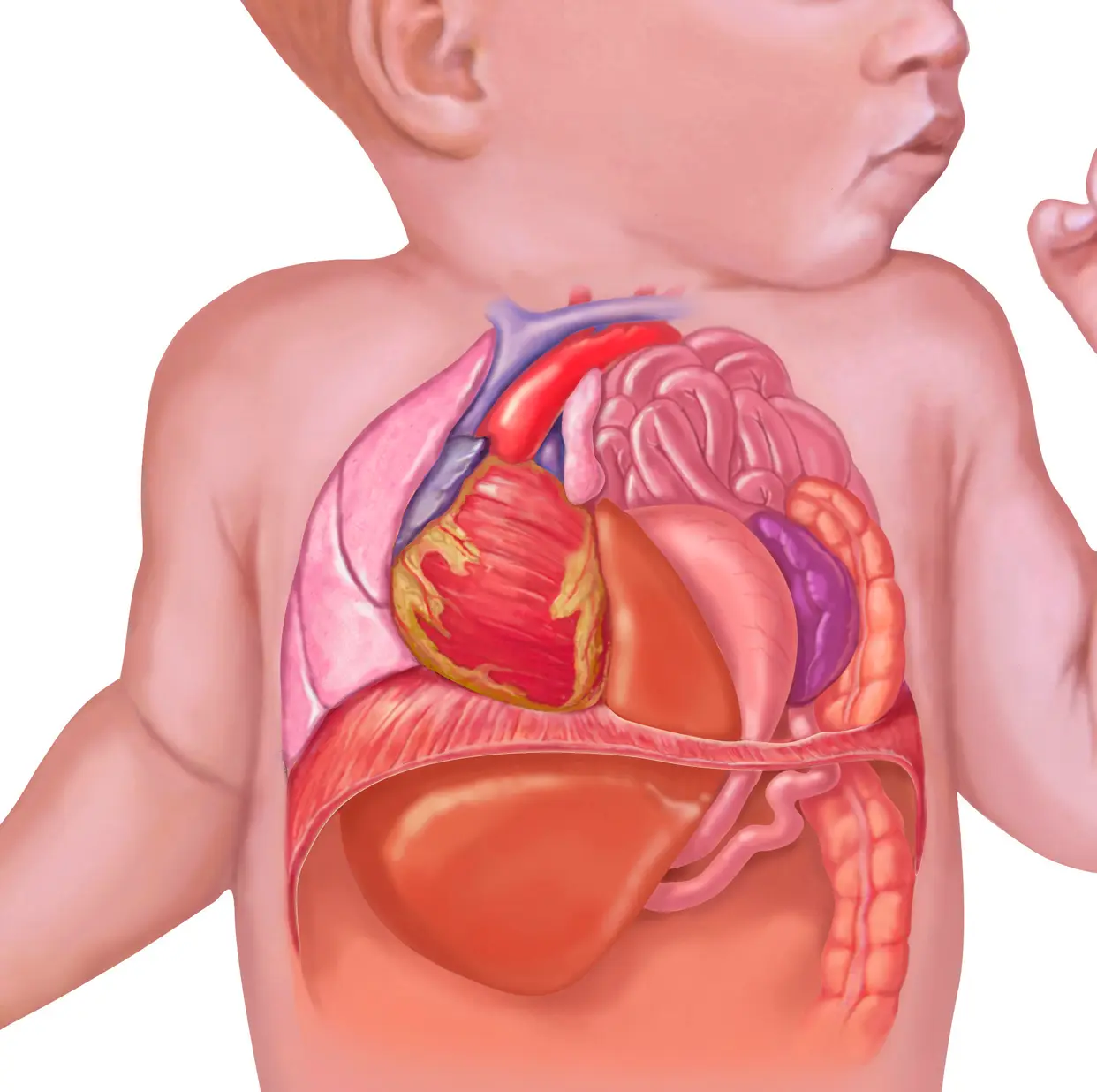
Congenital Morgagni’s hernia (CMH) is rare and represents less than 5% of all congenital diaphragmatic hernias. This is a national review of our experience with CMH outlining clinical presentation, methods of diagnosis, associated anomalies, treatment, and outcome.
Patients and methods
The medical records of all patients with the diagnosis of CMH treated at four pediatric surgery units in Saudi Arabia were retrospectively reviewed for age at diagnosis, sex, presenting symptoms, associated anomalies, diagnosis, operative findings, treatment, and outcome.
Results
During a 20-year period (January 1990–December 2010), 53 infants and children with CMH were treated. There were 38 males and 15 females. Their age at diagnosis ranged from 1 month to 9 years (mean 22.2 months). Forty-three (81%) presented with recurrent chest infection. Twenty-two (44.5%) had right CMH, 15 (28.3%) had left-sided hernia and 16 (30.2%) had bilateral hernia. In 7, the diagnosis of bilaterality was made at the time of surgery. Associated anomalies were seen in 38 (71.7%). Twenty-one (39.6%) had congenital heart disease, 8 (15%) had malrotation, and 15 (28.3%) had Down syndrome. All were operated on. Twenty-nine (54.7%) underwent repair via an open approach. The remaining 24 (45.3%) underwent repair using minimal invasive surgery, laparoscopic-assisted hernia repair (19 patients) or totally laparoscopic approach (5 patients). At the time of surgery, the hernia sac content included the colon in 33 (62.3%), part of the left lobe of the liver in 13 (24.5%), the small intestines in 11 (20.75%), the omentum in 5 (9.4%), and the stomach in 4 (7.5%). In 12 (22.6%), the hernia sac was empty. When compared to the open repair, the laparoscopic-assisted approach was associated with a shorter operative time, an earlier commencement of feeds, less requirement for postoperative analgesia, a shorter hospital stay, and better cosmetic appearance. There was no mortality. On follow-up, 2 (7%) of the open surgical group developed recurrence.
Conclusions
CMH is rare and in the pediatric age group commonly presents with recurrent chest infection and has a high incidence of associated anomalies, commonly congenital heart disease and Down syndrome. We advocate a laparoscopic-assisted approach to repair CMH. This is a simple technique that produces a sound repair, and when compared with the open approach it takes less operative time, requires less analgesia, allows earlier commencement of feeds, is associated with a shorter hospital stay, and has a better cosmetic outcome.